
Tags
American Academy of Orthopaedic Surgeons, Complication (medicine), Cutting, DePuy, Health, Hip Replacement, hip resurfacing, Invasiveness of surgical procedures, Medicine, Orthopedic surgery, Patient, surgery
Minimally Invasive Total Hip Arthroplasty
Author: Derek F Amanatullah, MS, MD, PhD; Chief Editor: Erik D Schraga, MD
Pre-procedure
Background
Minimally invasive total hip arthroplasty (MIS-THA) is often portrayed in the lay community and press as a small skin incision. MIS-THA is actually defined by limited soft tissue and bony dissection. Conventional THA is a successful operation for patients experiencing arthritis of the hip, with a reported complication rate of less than 2% and an implant survivorship of 95% at 10 years.[1]
 The major benefits of MIS-THA are patient perceived incisional cosmesis, psychological patient satisfaction, and possibly a shorter hospital stay.[2, 3, 4]With modern analgesia protocols, MIS-THA patients can often be discharged home within 24-48 hours postoperatively.[3, 4, 5] Decreased blood loss, decreased postoperative pain, and decreased need for postoperative ambulatory walking aids have also been reported with MIS-THA.[6]
The major benefits of MIS-THA are patient perceived incisional cosmesis, psychological patient satisfaction, and possibly a shorter hospital stay.[2, 3, 4]With modern analgesia protocols, MIS-THA patients can often be discharged home within 24-48 hours postoperatively.[3, 4, 5] Decreased blood loss, decreased postoperative pain, and decreased need for postoperative ambulatory walking aids have also been reported with MIS-THA.[6]
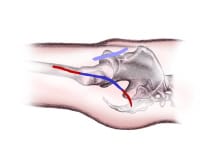
An image depicting minimally invasive total hip arthroplasty can be seen below.
 Incision comparison.Preoperative and postoperative gait analysis on 10 patients after mini-posterior THA demonstrated 85% recovery of gait velocity, a 90% recovery of single leg stance time, a 90% recovery of cadence, and a 70% return of stride length as well as less dependence on walking aids.[7] Moreover, 97% of MIS-THA patients were able to attain standard physical therapy goals (transferring in and out of bed from standing, rising from a chair to standing, moving from standing to sitting, walking 100 feet, and negotiating a full flight of stairs) within one day of surgery.[5]
Incision comparison.Preoperative and postoperative gait analysis on 10 patients after mini-posterior THA demonstrated 85% recovery of gait velocity, a 90% recovery of single leg stance time, a 90% recovery of cadence, and a 70% return of stride length as well as less dependence on walking aids.[7] Moreover, 97% of MIS-THA patients were able to attain standard physical therapy goals (transferring in and out of bed from standing, rising from a chair to standing, moving from standing to sitting, walking 100 feet, and negotiating a full flight of stairs) within one day of surgery.[5]
However, other studies have found no differences in operative time, pain control, transfusion rates, estimated blood loss, operative time, length of hospital stay, gait (ie, stride length, cadence, or walking speed), or Harris Hip Score.[8, 9, 10, 11, 12]
Indications
Conflicting data and no definitive answer exists regarding whether MIS-THA is an acceptable replacement or even an improvement on conventional THA.
Contraindications
No absolute contraindications exist to MIS-THA; it is defined by limited soft tissue and bony dissection. Patients with a BMI greater than 30 kg/m2, severe osseous dysplasia (eg, superior femoral head migration), revision THA, and severe hip contracture or patients who are exceedingly muscular are probably better suited for conventional THA.[3, 7, 13]
Preparation
The preoperative evaluation and preparation for a MIS-THA is exactly the same as for conventional THA, except for specialized surgical instrumentation and implants. Since exposure may be limited, MIS-THA may require modification of conventional instrumentation and possibly additional equipment (eg, fiberoptic light cables, cutaway reamers, Hohmann retractors with light sources, flexible acetabular reamers).[14, 15, 16]
 Using particular operating room tables make certain MIS-THA approaches more accessible and may be required to provide requisite traction and permit rotation of the lower extremity. A Judet Orthopaedic Table (Tasserit, Sens, France) or a PROfx Fracture Table (OSI, Union City, CA) can be used with an anterior approach, and the Jupiter Table (Trumpf, Charleston, SC) with the anterolateral approach.[15, 17, 18]
Using particular operating room tables make certain MIS-THA approaches more accessible and may be required to provide requisite traction and permit rotation of the lower extremity. A Judet Orthopaedic Table (Tasserit, Sens, France) or a PROfx Fracture Table (OSI, Union City, CA) can be used with an anterior approach, and the Jupiter Table (Trumpf, Charleston, SC) with the anterolateral approach.[15, 17, 18]
Another unique aspect of MIS-THA is that preoperative templating can guide component and incision size. For example, a 4-inch incision would be appropriate for inserting a size 56 acetabular component while avoiding contact between the prosthesis and skin or subcutaneous fat.[2] A double-blinded randomized controlled trial identified a doubling of the risks associated with the MIS-THA with a surgeon’s first 60 MIS-THA cases, but this increased risk was not present with a surgeon’s next 60 MIS-THA cases.[19] This data gives some idea of a learning curve associated with MIS-THA and suggests surgeons not undertake MIS-TKA without appropriate training and mentorship.
Complication Prevention
Complication prevention for a MIS-THA is exactly the same as for conventional THA and should include appropriate preoperative screening and clearance, preoperative templating and planning, and preoperative administration of antibiotics as recommended by the American Academy of Orthopaedic Surgeons.
Technique
Approach
Among the first alternatives to the transtrochanteric approach to the hip were the conventional posterior and lateral approaches.[20] These early alternative approaches sought to limit disturbance to osseous and soft tissue anatomy, thereby avoiding unnecessary complications such as trochanteric nonunion.[21, 22] The conventional posterior and lateral approaches were nevertheless reported to be associated with gluteal nerve injuries.[23]
Beginning in the 1990s, these conventional surgical approaches were further modified to limit soft tissue dissection and avoid damage to healthy surrounding structures. Minimally invasive total hip arthroplasty (MIS-THA) is actually a broad term encompassing multiple mini-surgical approaches. A single mini-incision approach is usually less than 10 cm in length, while a 2-incision approach usually has 2 incisions, each less than 5 cm in length (see the image below).
Incision comparison.The posterior approach is the workhorse approach for conventional THA.[20]The mini-posterior approach uses the same plane of dissection as the conventional posterior approach but minimizes the soft tissue dissection.[16, 24] The gluteus maximus split should be kept to a minimum, and release of the gluteus maximus tendon insertion should be avoided. An anterior capsular release is critical. Releasing the anterior capsule facilitates femoral mobilization and easy delivery of the femur into a small wound.[14] Lastly, a meticulous posterior capsular closure with short rotator reattachment is critical to the mini-posterior and conventional posterior approaches, because it reduces the risk of postoperative dislocation risk from 3% to 0.85%.[25]
The anterior approach uses the internervous plane between femoral nerve (lateral border of the sartorius and rectus femoris muscles) and superior gluteal nerve (medial border of the tensor fascia latae and gluteus medius muscles). Because no muscle needs to be split or tendon needs to be cut, it represents the optimal mini-incision approach.[7, 17]
For the posterolateral approach, an incision is made over the posterior aspect of the greater trochanter, and the gluteus medius and minimus are elevated off of the capsule.[26]
For the lateral approach, the skin incision runs from 2 cm proximal to the greater trochanter to 5-8 cm distally along a line parallel to the long axis of the femur. After incising the tensor fasciae latae, the gluteus medius fibers are cut to expose the joint capsule.[27]
The skin incision for the anterolateral approach goes from the anterior tubercle of the greater trochanter and angles toward the anterior superior iliac spine. Like the anterior approach, it uses the interval between the gluteus medius and tensor fasciae latae and usually only requires elevating the anterior one-third of the gluteus medius.[15, 26] A possible downside to the anterolateral approach is transection of the superior gluteal nerve.[28]
The 2-incision approach consists of a 5 cm anterior incision directly over the femoral neck used for accessing the acetabulum and inserting the cup and a 3 cm posterior incision in line with the femoral canal used for the femoral preparation. The anterior approach uses the internervous plane between the femoral and superior gluteal nerves, and the posterior approach uses the plane between the abductor tendons anteriorly and the piriformis posteriorly.[7] Some authors recommend using fluoroscopy to verify the correct location of the skin incisions, while others feel like this extra equipment is not necessary.[16, 29]
Techniques
The femoral neck may need to be osteotomized in situ or piecemeal instead of dislocating the hip and removing the femoral head en bloc.[5, 15]
Post-Procedure
Complications
Despite the portrayal of minimally invasive totaly hip arthroplasty (MIS-THA) as a small cosmetically pleasing skin incision, plastic surgeons rated 6 of 20 MIS-THA scars as poor and only 1 of 14 conventional THA scars as poor. Thirty of 31 of those same patients also stated that pain relief and implant longevity were more important than scar cosmesis after 2 years of follow-up.[30]
MIS-THA is associated with a 6% increase in local wound complications.[9]This may be secondary to increased soft tissue and cutaneous trauma from the retraction or reamers abrading the skin.[31] However, 2 meta-analyses showed this increase is not statistically significant.[11, 12]
Damage to surrounding structures, especially nerves, is one of the main concerns with MIS-THA. The anterolateral approach places the superior gluteal nerve at significant risk, as 4 of 5 were cut during a cadaveric study.[28] A meta-analysis demonstrated a 5-fold increase in the risk of LFCN palsy after MIS-THA, as well as a statistically significant increased risk for any nerve palsy.[12]
Other surgical complications of MIS-THA include proximal femoral fracture (2.8% for 2-incision approach), hematoma (2% from one study), acetabular component malposition (an abduction angle of less than 35° or greater than 50° was seen in 4% and 11%, respectively, using the posterolateral approach), and varus femoral component malposition (14% using the posterior approach).[3, 7, 9, 32] Acetabular cup anteversion was 3 times more likely to be outside the acceptable range with the posterior and posterolateral MIS-THA approaches.[33]
Since the posterior approach is associated with increased risk of posterior dislocation, it is reasonable to continue to expect this as a potential complication. However, one study of 1,000 hips using the mini-posterior technique reported a posterior dislocation rate of 1.2%, which is less than the value of 5.8% reported using the standard posterior approach.[13, 34] Despite sufficient soft tissue mobilization in properly selected patients, limited surgical visualization may necessitate conversion of the MIS-THA incision into a more conventional THA approach in less than 10% of patients.[27]
The two-incision approach uses unique dissection planes; as a result, it has a significant learning curve resulting in a higher than expected complication rate.[35] The rate of complications did not decrease over a surgeon’s first 10 cases, suggesting that a longer learning curve than expected exists.[36] The 2-incision MIS-THA is supposed to spare cutting muscles and tendons, although cadaveric studies of 10 hips showed that in every case the abductors, external rotators, or both were injured.[37] Moreover, unlike standard mini-incision approaches to the hip, which use large dissection planes, the 2-incisions have limited extensibility. As a result of the increased level of skill and experience required to perform this approach safely and correctly, many surgeons feel that this approach is best performed by high-volume surgeons who receive specialized training.[7]
Long-term Monitoring
Patients should be followed at the same time interval as a conventional THA with periodic clinical and radiographic examinations to monitor for aseptic loosening and late infection.
Patient Education
Patient education prior to conventional and MIS-THA with respect to postoperative expectations as well as the administration of anticoagulation are imperative. Counseling with respect to activity level is left to the discretion of the surgeon.
References
- Havelin LI, Engesaeter LB, Espehaug B, Furnes O, Lie SA, Vollset SE. The Norwegian Arthroplasty Register: 11 years and 73,000 arthroplasties. Acta Orthop Scand. Aug 2000;71(4):337-53. [Medline].
- Goldstein WM, Branson JJ. Posterior-lateral approach to minimal incision total hip arthroplasty. Orthop Clin North Am. Apr 2004;35(2):131-6. [Medline].
- Howell JR, Masri BA, Duncan CP. Minimally invasive versus standard incision anterolateral hip replacement: a comparative study.Orthop Clin North Am. Apr 2004;35(2):153-62. [Medline].
- Berger RA. Total hip arthroplasty using the minimally invasive two-incision approach. Clin Orthop Relat Res. Dec 2003;(417):232-41.[Medline].
- Berger RA. The technique of minimally invasive total hip arthroplasty using the two-incision approach. Instr Course Lect. 2004;53:149-55. [Medline].
- Wright JM, Crockett HC, Delgado S, Lyman S, Madsen M, Sculco TP. Mini-incision for total hip arthroplasty: a prospective, controlled investigation with 5-year follow-up evaluation. J Arthroplasty. Aug 2004;19(5):538-45. [Medline].
- Berry DJ, Berger RA, Callaghan JJ, Dorr LD, Duwelius PJ, Hartzband MA. Minimally invasive total hip arthroplasty. Development, early results, and a critical analysis. Presented at the Annual Meeting of the American Orthopaedic Association, Charleston, South Carolina, USA, June 14, 2003. J Bone Joint Surg Am. Nov 2003;85-A(11):2235-46. [Medline].
- de Beer J, Petruccelli D, Zalzal P, Winemaker MJ. Single-incision, minimally invasive total hip arthroplasty: length doesn’t matter. J Arthroplasty. Dec 2004;19(8):945-50. [Medline].
- Woolson ST, Mow CS, Syquia JF, Lannin JV, Schurman DJ. Comparison of primary total hip replacements performed with a standard incision or a mini-incision. J Bone Joint Surg Am. Jul 2004;86-A(7):1353-8. [Medline].
- Ogonda L, Wilson R, Archbold P, et al. A minimal-incision technique in total hip arthroplasty does not improve early postoperative outcomes. A prospective, randomized, controlled trial. J Bone Joint Surg Am. Apr 2005;87(4):701-10. [Medline].
- Reininga IH, Zijlstra W, Wagenmakers R, et al. Minimally invasive and computer-navigated total hip arthroplasty: a qualitative and systematic review of the literature. BMC Musculoskelet Disord. May 17 2010;11:92. [Medline]. [Full Text].
- Smith TO, Blake V, Hing CB. Minimally invasive versus conventional exposure for total hip arthroplasty: a systematic review and meta-analysis of clinical and radiological outcomes. Int Orthop. Feb 2011;35(2):173-84. [Medline]. [Full Text].
- Sculco TP, Jordan LC, Walter WL. Minimally invasive total hip arthroplasty: the Hospital for Special Surgery experience. Orthop Clin North Am. Apr 2004;35(2):137-42. [Medline].
- Sculco TP, Jordan LC. The mini-incision approach to total hip arthroplasty. Instr Course Lect. 2004;53:141-7. [Medline].
- Bertin KC, Rottinger H. Anterolateral mini-incision hip replacement surgery: a modified Watson-Jones approach. Clin Orthop Relat Res. Dec 2004;248-55. [Medline].
- Scuderi GR, Tenholder M, Capeci C. Surgical approaches in mini-incision total knee arthroplasty. Clin Orthop Relat Res. Nov 2004;61-7. [Medline].
- Siguier T, Siguier M, Brumpt B. Mini-incision anterior approach does not increase dislocation rate: a study of 1037 total hip replacements. Clin Orthop Relat Res. Sep 2004;164-73. [Medline].
- Woolson ST, Pouliot MA, Huddleston JI. Primary total hip arthroplasty using an anterior approach and a fracture table: short-term results from a community hospital. J Arthroplasty. Oct 2009;24(7):999-1005. [Medline].
- Goosen JH, Kollen BJ, Castelein RM, Kuipers BM, Verheyen CC. Minimally invasive versus classic procedures in total hip arthroplasty: a double-blind randomized controlled trial. Clin Orthop Relat Res. Jan 2011;469(1):200-8. [Medline]. [Full Text].
- Jolles BM, Bogoch ER. Posterior versus lateral surgical approach for total hip arthroplasty in adults with osteoarthritis. Cochrane Database Syst Rev. 2004;CD003828. [Medline].
- Bergstrom B, Lindberg L, Persson BM, Onnerfalt R. Complications after total hip arthroplasty according to Charnley in a Swedish series of cases. Clin Orthop Relat Res. Sep 1973;91-5. [Medline].
- Amstutz HC, Maki S. Complications of trochanteric osteotomy in total hip replacement. J Bone Joint Surg Am. Mar 1978;60(2):214-6.[Medline].
- Abitbol JJ, Gendron D, Laurin CA, Beaulieu MA. Gluteal nerve damage following total hip arthroplasty. A prospective analysis. J Arthroplasty. Dec 1990;5(4):319-22. [Medline].
- GIBSON A. Posterior exposure of the hip joint. J Bone Joint Surg Br. May 1950;32-B(2):183-6. [Medline].
- Weeden SH, Paprosky WG, Bowling JW. The early dislocation rate in primary total hip arthroplasty following the posterior approach with posterior soft-tissue repair. J Arthroplasty. Sep 2003;18(6):709-13. [Medline].
- Blasser K. Advances in Total Hip Replacement: Minimally Invasive Surgery. Northeast Florida Medicine. 2006;57(3).
- Ilizaliturri VM Jr, Chaidez PA, Valero FS, Aguilera JM. Small incision total hip replacement by the lateral approach using standard instruments. Orthopedics. Apr 2004;27(4):377-81. [Medline].
- van Oldenrijk J, Hoogland PV, Tuijthof GJ, Corveleijn R, Noordenbos TW, Schafroth MU. Soft tissue damage after minimally invasive THA. Acta Orthop. Dec 2010;81(6):696-702. [Medline].
- Kennon RE, Keggi JM, Wetmore RS, Zatorski LE, Huo MH, Keggi KJ. Total hip arthroplasty through a minimally invasive anterior surgical approach. J Bone Joint Surg Am. 2003;85-A Suppl 4:39-48. [Medline].
- Mow CS, Woolson ST, Ngarmukos SG, Park EH, Lorenz HP. Comparison of scars from total hip replacements done with a standard or a mini-incision. Clin Orthop Relat Res. Dec 2005;441:80-5. [Medline].
- Kiyama T, Naito M, Shitama H, Shinoda T, Maeyama A. Comparison of skin blood flow between mini- and standard-incision approaches during total hip arthroplasty. J Arthroplasty. Oct 2008;23(7):1045-9. [Medline].
- Hartzband MA. Posterolateral minimal incision for total hip replacement: technique and early results. Orthop Clin North Am. Apr 2004;35(2):119-29. [Medline].
- Cheng T, Feng JG, Liu T, Zhang XL. Minimally invasive total hip arthroplasty: a systematic review. Int Orthop. Dec 2009;33(6):1473-81.[Medline]. [Full Text].
- Woo RY, Morrey BF. Dislocations after total hip arthroplasty. J Bone Joint Surg Am. Dec 1982;64(9):1295-306. [Medline].
- Pagnano MW, Leone J, Lewallen DG, Hanssen AD. Two-incision THA had modest outcomes and some substantial complications. Clin Orthop Relat Res. Dec 2005;441:86-90. [Medline].
- Archibeck MJ, White RE Jr. Learning curve for the two-incision total hip replacement. Clin Orthop Relat Res. Dec 2004;232-8.[Medline].
- Mardones R, Pagnano MW, Nemanich JP, Trousdale RT. The Frank Stinchfield Award: muscle damage after total hip arthroplasty done with the two-incision and mini-posterior techniques. Clin Orthop Relat Res. Dec 2005;441:63-7. [Medline].
Related articles
- Techniques In Implementing A Hip Replacement Operation (earlsview.com)
- Hematoma prevention important in reducing morbidity, mortality from THA (earlsview.com)
- My Revision is Planned for 1 September – Yahoo!!! (earlsview.com)
- How Long Do Hip Replacements Last? (earlsview.com)
- MHRA Advice for Patients (earlsview.com)
- Associate Professor Michael J. Neil – Doesn’t Recommend Resurfacing (earlsview.com)
Pingback: Advances in Knee Replacement Surgery for Active Baby Boomers « Earl's View
Pingback: Smoking Tied to Increase in Post-Arthroplasty Complications – Bugger!!! « Earl's View
Pingback: Fast Track Total Hip Replacement Surgery « Earl's View
Pingback: Hip Resurfacing has Higher Risk of Revision « Earl's View
Pingback: Make Sure You DON’T get the Wrong Surgery… « Earl's View
Pingback: Expert Advisory Group looking at soft tissue reactions associated with metal-on-metal hip replacements « Earl's View
Pingback: Longer Cemented Stems Better in Hip Revisions « Earl's View
Pingback: Hip Dislocations – Why? « Earl's View
Pingback: Viles & Beckman, LLC; Summary of Hip Replacement Defects « Earl's View
Pingback: Staple Closure – Greater Than 3 Times The Risk of Infection « Earl's View
Pingback: Bone Cements – Not all Work Well « Earl's View
Pingback: Pseudotumors in MoM Hip Replacements « Earl's View
Pingback: Anterior Hip Replacements are the Future « Earl's View
Pingback: Zimmer NexGen CR-Flex Porous Femoral Component Complaints « Earl's View
Pingback: Cementless Implants Tied to Improved Hip Implant Survival « Earl's View
Pingback: Recovery Benefit of MIS THA to Give a Faster Functional Recovery Not Proven « Earl's View
Pingback: Hip Resurfacing – Dancer Back at Rehersals after 7 Months « Earl's View
Pingback: Extracts from Australian Orthopaedic Association National Joint Replacement Registry – Annual Report 2010 « Earl's View
Pingback: New Zealand National Joint Registry Eleven Years Data Jan 1999 – 2009 « Earl's View
Pingback: Anterior Hip Replacement « Earl's View
Pingback: Age, surgery type, coronary artery disease associated with complications after TKA « Earl's View
Pingback: Operative time, use of biological agents increase risk of complications following TKA « Earl's View
Pingback: American Joint Replacement Registry (AJRR) completes data collection pilot project « Earl's View
Pingback: UK – Advice for GP’s – Hip Joint Replacements « Earl's View
Pingback: Hip Dysplasia – all you didn’t want to know! « Earl's View
Pingback: Hypertensive Patients Show Delayed Wound Healing following Total Hip Arthroplasty « Earl's View
Pingback: New Hips Gone Awry Expose U.S. Kickbacks in Doctors’ Conflicts « Earl's View
Pingback: Coloarticular fistula: A rare complication of revision total hip arthroplasty « Earl's View
Pingback: Length of stay following Total Hip Repalcement multifactorial, study finds « Earl's View
Pingback: Obesity a significant risk factor in complication rates following THA « Earl's View
Pingback: Femoral Osteotomy – commonly used for adults in the treatment of hip fracture nonunions and malunions « Earl's View
Pingback: Femoral Osteotomy Treatment & Management « Earl's View
Pingback: THA after intertrochanteric osteotomy results in higher complication rates, lower long-term prosthesis survival rates « Earl's View
Pingback: Supervised Exercise With Hip Osteoarthritis Allows Patients to Delay Total Hip Replacement « Earl's View
Pingback: Novel Oral Anticoagulants for VTE Prevention in Orthopedic Surgery: Overview of Phase 3 Trials « Earl's View
Pingback: Study: Two-day Discharge After Arthroplasty Feasible « Earl's View
Pingback: Mini bus hire in St5 3jh : Coach Hire in St5 3jh